My Saturday weigh-in was, on the surface, a little disappointing. My weight had fluctuated up this week, with Tuesday’s weigh-in showing a completely unexpected 3.1 lbs / 1.4 kg increase!
While I did cut my Monday 36-hour fast short, I had two 36hr fasts the previous week, and stuck to strict keto principles – as well as increasing my swimming, running, and introducing cycling and more mobility and strength work! So, a weight gain was not something I had factored in at all! But maybe I should have.
As we’ve discussed before, the body is not a simple machine of inputs and outputs – it’s a complex metabolic maze – a puzzle at times. While on paper I am maintaining a calorie deficit, I’m also increasing exercise, which requires muscle repair, which in turn requires water.
Think of it like building a wall. 🧱
You need bricks (essential proteins), sand, and cement (the hormonal signals and micronutrients that bind it all together), and also water to get the right consistency. So the body retains extra water to build the muscle.
It takes energy to put up the brickwork, and likewise, it takes energy to build muscle. But how is that possible if I’m fasting and therefore at a calorie deficit? There’s a common misconception that you have to be in a calorie surplus / excess in order to build muscle, but that’s simply not the case. As long as you have fuel and the right building blocks you can build muscle.
We use fat to fuel everyday bodily functions during ketosis, and we use the same fat to build the wall, which increases the deficit.
Only once the muscle is built is any excess water released. But since we’re tearing down the walls and building new ones (more exercise, resulting in stronger, more efficient muscles) every week, the body is never too eager to let go of its building materials.
“Muscle is heavier than fat”…isn’t it?
We often hear that ‘muscle weighs more than fat,’ but of course that’s nonsense – a pound of feathers weighs the same as a pound of iron!🪶⚖️
But it is true that muscle is denser than fat. Almost 20% denser, so muscle on your body takes up 20% more space than your body fat did. That is why my jeans are falling off me even though the scale is holding steady at 99.6kg!
Plus, there’s a massive metabolic cheat code here: muscle is active tissue. Every pound of muscle I build burns about three times more calories at rest than fat does. By trading fat for muscle, I’m building a bigger, hungrier engine that burns calories even while I sleep.
The mirror, tape, and scale
When we exercise while also maintaining a calorie deficit, it’s therefore important that we relegate the scale to more of a general guideline.
The mirror and the measuring tape are more reliable sources of data than our body weight. As we’ve seen in the past, my weight fluctuates a lot, even over a day or two, far more than is possible due to fat gain and loss. I “gained” 3.1 lbs / 1.4 kg in just 3 days, then “lost” 2.3 lbs / 1 kg in four days. Neither fat nor muscle are gained or lost that rapidly.
What we’re doing when we exercise is not about weight loss, it’s about body recomposition. We are literally converting body fat into muscle, and that requires water, which CAN fluctuate hugely over the course of a few hours let alone days.
So over time, there will definitely be a net loss in weight, as we lose fat and turn it into muscle, which in turn burns more energy – but while we’re rebuilding, the scales might tell us otherwise.
What I’ve really noticed this week is how much better I look in the mirror. I can see my abs and oblique muscles starting to show, and a lot more size as well as definition in my legs.
So, the net result of this week’s recomposition effort is that I’m back down to 15st 9.5lbs (219.5lb/99.6kg). So I’m still under that 100kg mark, but also a much more svelte-looking version!
Progress Update: May 9, 2026
Week 20
HbA1c: 42 mmol/mol
Remission as of 30/03/2026
15 St 9.5 lbs
219.5 lbs / 99.6kg
Total loss (since December): 2st 10.4lbs (38.4lb/17.4kg)
Total loss (since Diagnosis): 3st 4lbs (46lb/20.9kg)
Exercise
Monday:
None
Bank Holiday brain fart!
Tuesday:
Swim: 1 x 750m, 1 x 500m, 1 x 250m (1.5km)
Mile swim!
Wednesday:
Run: 6×2.5min run / 1 min walk
Solid run
Thursday:
Cycle: 30 min / 10km easy, Swim: 4x250m (1km)
Easy bike ride and recovery swim
Friday:
Run: 2 min run, 1 min walk, GMB Fitness Mobility 15 mins
TBD
Saturday:
Swim: 1 x 750m, 1 x 500m, 1 x 250m (1.5km)
TBD !
Fasting
Monday:
24 hr fast
Caved
Wednesday:
40 hr fast
Completed second fast of the week successfully
Friday:
36 hr fast
Completed 3rd fast of the week successfuly!
Blood Pressure
Tuesday:
AM 148/97 PM 148/88 (66bpm)
BP very high during GP appt so asked to keep BP diary
Wednesday:
AM 135/88 (61 bpm) PM 137/80 (72 bpm)
Definitely better today
Thursday:
AM 144/92 (67 bpm) PM 119/85 (75 bpm)
High this morning but amazing this evening!
Friday:
AM 143/92 (62 bpm) PM 129/88 (67 bpm)
Once again, high in the morning, but pretty good in the evening
Saturday:
AM 127/84 (61 bpm) PM xx/xx (xx bpm)
Amazing morning reading, one of my best!
Target: 12st 12 lbs (180lbs / 82kg)
Remaining: 39.5 lbs / 17.9kg
54%
Anyway, I’m going to worry less about the scales, and more about my recomposition efforts – plenty of high-quality protein, lots of exercise, intermittent fasting, and plenty of rest. The rest will take care of itself.
Following my diabetic check-up on Tuesday, my clinician asked me to keep a week-long morning and evening BP diary. It has been an incredibly eye-opening exercise.
Normally, I only test in the morning. But looking at the full day’s data, I realized my morning readings are heavily impacted by the “morning surge.” As we wake up, our systems are flooded with cortisol to wake us up, which often leads to elevated readings.
Throughout the day, my vascular system is actually in much better shape than I thought!
The Big Takeaways:
The “Initial shock”: My first reading is almost always high (constricted vessels). This can be caused by the very mild shock of just putting the BP cuff on and thinking about the logistics of taking the reading, but also demonstrates I’m usually not fully relaxed. By the second or third reading, it drops significantly.
Exercise is Medicine: On Thursday, after my bike ride, my BP dropped to 120/76—literally a normal, healthy reading!
The Ultimate Morning Victory: This Saturday morning, I hit a resting average of 120/80 with a resting pulse of 60 bpm! For my age and where I started, that is incredible.
So, I finally got my results back from my HbA1c after my interim diabetic checkup, and it wasn’t great news.
As I’ve discussed, having dropped from a dangerously high blood sugar reading of 79 mmol/mol (9.4%) in December to an amazing 42 (6.0%) on 30th March, I was fully expecting to have continued on that same trajectory, which would have taken me down to the mid 30s in mmol/mol (5.3-5.6%)!
Best case, I was hoping maybe to be even in the early 30’s (5.0-5.2%). A very optimistic part of me was hoping that I’d hit the late 20’s (4.6-4.8%), taking me very close to my ultimate goal which is a “normal/healthy” A1c!
So I was really quite crestfallen to see my new number was 40 (5.8%)! Just 2 points down from my last test which was six weeks before.
Now, it must be said that in that period, I had a couple of pretty bad “cheat days” – one just aroudn ten days before my test – and the way the HbA1c test works, it does “prioritise” the more recent results. But it was just one or two meals out of six weeks, in which I was still fasting for 36hrs three days a week, eating strict keto and had increased my exercise to a solid 6 days a week pretty consistently.
Still, it’s a bit of a surprise, and not a good one.
The one thing I have to remember is that the HbA1c is just an average. I only realised after recently joining some diabetic Facebook groups that most diabetics test their blood sugar throughout the day, and so I’m getting myself a cotinuous glucose monitor – this is a sensor that attaches to your arm and reads your blood sugar continuously (hence the name! 🤪) throughout the day and sends the results in near real time to your phone.
This will give me a much more accurate picture of what my blood sugar is actually doing to keep me from dropping my number more rapidly.
I finally got back on the saddle this week! After losing some gear during the Cambridgeshire move and replacing a damaged helmet, there were no more excuses.
I plotted a “cycle-friendly” route on my Garmin, but 15 minutes in, the road literally ended at a gated private farm. I had to pivot (literally, turn around and go back the way I came!😜), but it was still a great 30-minute, 10km ride to blow off the cobwebs. Best of all? I was 38 hours into a fast and felt fantastic.
I also fit in my recovery swim later that afternoon. I’m working on bilateral breathing (taking 5 strokes instead of 3 between breaths), which is a work in progress, but the core/upper body focus felt great after the morning cycle.
The Protein Focus
Fasting for 36 hours and exercising twice a day means I really have to think about my nutrition on feeding days. I’ve been worried I’m not getting enough protein in particular, so I’m making a conscious effort to ramp it up:
Breakfast: A massive 4-egg omelette with red onion, mushrooms, avocado, 3 chicken chipolatas, and nitrate-free bacon.
Afternoon: A Greek yogurt and keto granola smoothie boosted with an extra half-scoop of whey protein.
Dinner: 650g of diced chicken breast air fried in Korean spices served with broccoli, cauliflower and spinach. The chicken was actually so much I had to split it over a “main meal” and then a late snack!
When you’re doing a metabolic reset like this – losing 40lbs in 100 days via a combination of strict keto diet, intermittent fasting, and exercise – people (and doctors!) often worry about the strain on your body. They wonder if the kidneys are holding up or if your electrolytes are crashing.
The results are in, and it’s a clean sweep!
Kidney Function: My filtration rate (eGFR) is exactly where it should be – operating at peak performance.
Electrolytes: My sodium, potassium, and chloride levels are rock-solid. This is a huge win because it proves that my hydration and mineral balance are perfect, even with the fasting and keto protocol.
Hydration & Metabolism: My urea and creatinine levels show that my body is processing everything smoothly without any signs of dehydration or stress.
The Takeaway: This “mini-win” is actually a major milestone for me. It proves that this isn’t just about “starving the sugar” – it’s about a healthy, sustainable biological shift. My “engine” isn’t just surviving this challenge; it’s thriving.
Stay tuned… the official HbA1c should be here any moment! 🤞
What a weird start to the week! After driving back from Newcastle on Monday, I was feeling great – until I tried to do my usual routine. I got fully prepped for my swim, drove to the pool, and found… a dark, deserted building. Then I drove to Tesco for groceries. Closed.
Mental note: Always remember UK Bank Holidays. 😅
Ending up back home early, and settling in to watch a movie, triggered my old movie-watching snack habits, and I wound up breaking my 36-hour fast early at the 24-hour mark (pork crackling and cream cheese to keep it keto). I’m not beating myself up though – redundancy anxiety is real and ongoing, and sometimes you just have to adapt.
The Tuesday Comeback
I carried my missed Monday swim over to Tuesday lunchtime, and wow, what a session. I felt so good during my first 500m that I pushed it to a 750m set (half a mile non-stop!). My shoulder warned me not to go too crazy on the second set, so I did a 500m, rested and stretched my shoulders out, and then finished with a final 250m.
Total distance: 1.5km – the Swimmer’s Mile! 🥳
That’s a great comeback from a ditzy Monday brain-fart to a personal Tuesday milestone – emphasis on the mile, obviously! 😆.
So, I finallyhad my long overdue diabetic check-up today – just a weigh-in, blood pressure check and drawing blood for my “quarterly” HbA1c check-up.
Regular followers will remember that I was due my check-up on 27th March, but it got postponed the day before and rescheduled until today (5th May)! Much to my chagrin as I was really excited to see how my HbA1c looked after three months on my aggressive Type 2 diabetes remission program.
So I went ahead and ordered my own private HbA1c test from MonitorMyHealth, a highly reputable and reliable private service here in the UK, notably because they use the same NHS labs that UK GP surgeries use. It was actually MonitorMyHealth who provided my initial diagnosis of Type 2 Diabetes two and a half years ago.
Anyway, the results from that test were far beyond my wildest dreams – I had been at 79 mmol/mol (9.4%) at my previous test in December – well into the “seriously uncontrolled diabetes” zone, and had just started to experience some more severe symptoms.
I had been expecting a result in the early 50’s (6.8-7.1%). Secretly hoping for 48 mmol/mol (6.5%). And hoping against hope for something even lower.
42-48 (6.0-6.5%) is classed as “prediabetes” and getting to 48 or below is the target most clinicians give their Type 2 patients in the first instance. Getting to 48 and under, and maintaining that for six months without medication, is the UK medical system’s classification for “remission”.
Anyway, I smashed my target and went straight to the bottom end of the prediabetic range at 42 mmol/mol (6.0%)! I was over the moon! And so today I was naturally very excited to see my diabetic clinician and show off my results.
I don’t think she believed what I was showing her, she was so flabbergasted. She was also shocked by my weight loss – since I’ve now lost nearly 18% of my diagnosis weight, more than 1/6th and approaching 1/5th of my original body weight!
When I explained my regimen to her, she was also quite taken aback.
The biggest surprise came when I told her I am only half way to my weight-loss target, and that I am also targeting an HbA1c around 23-27 mmol/mol (4.3%–4.6%) , which is the absolutely optimum range for health, the level of a healthy child or an adult athlete. She actually laughed! She said “very few people have an A1c in that range”.
“very few people have an A1c in that range”. Diabetes specialist clinician, on my goal to achieve an optimal HbA1c of 23-27 mmol/mol (4.3%-4.6%)!
Wow! I mean, I guess I shouldn’t be surprised – we live in a society where diets are simply awful. Even the “healthiest” people are likely eating a lot of processed junk. But if “very few people” are in that optimal, healthy range, that effectively means most are on their way towards Type 2 Diabetes. Of course, many may be able to keep it under control, but clearly, many eventually succumb.
The current statistics from Diabetes UK state that 1 in 9 people are living with undiagnosed “prediabetes” right now. And of course, I was one of them. When I think back now to the years before my diagnosis, the signs were all there. It’s such a shame that most people are blissfully unaware and seem to think diabetes is something that happens to other people!
Clearly, if “optimal health” from a blood sugar perspective is so rare it suggests that number will only continue to grow. But it is disconcerting. And really disconcerting for an experienced medical professional to be so resigned to sub-optimal health, and so dismissive of someone progressing towards it!
But don’t worry – I didn’t take it to heart. Not one bit. What I heard was not a negative at all. What I heard was a clear challenge. I don’t want to just live with prediabetes, or even “normal” blood sugar. I don’t want to be “sub-optimal” anymore.
If there is an optimal number for health and longevity, then that is where I’m heading.
So – challenge accepted!
Meanwhile, watch this space over the next day or so – I’ll get my new updated HbA1c test results back shortly, and I’m excited to see how far along I am. My last test was just over five weeks ago now, and assuming I’ve kept along roughly the same trajectory, I should now be in the mid 30s in mmol/mol (5.3-5.6%)! Best case, even the early 30’s (5.0-5.2%). I don’t dare hope (do I dare??) that I’ll hit the late 20’s (4.6-4.8%)! 😜
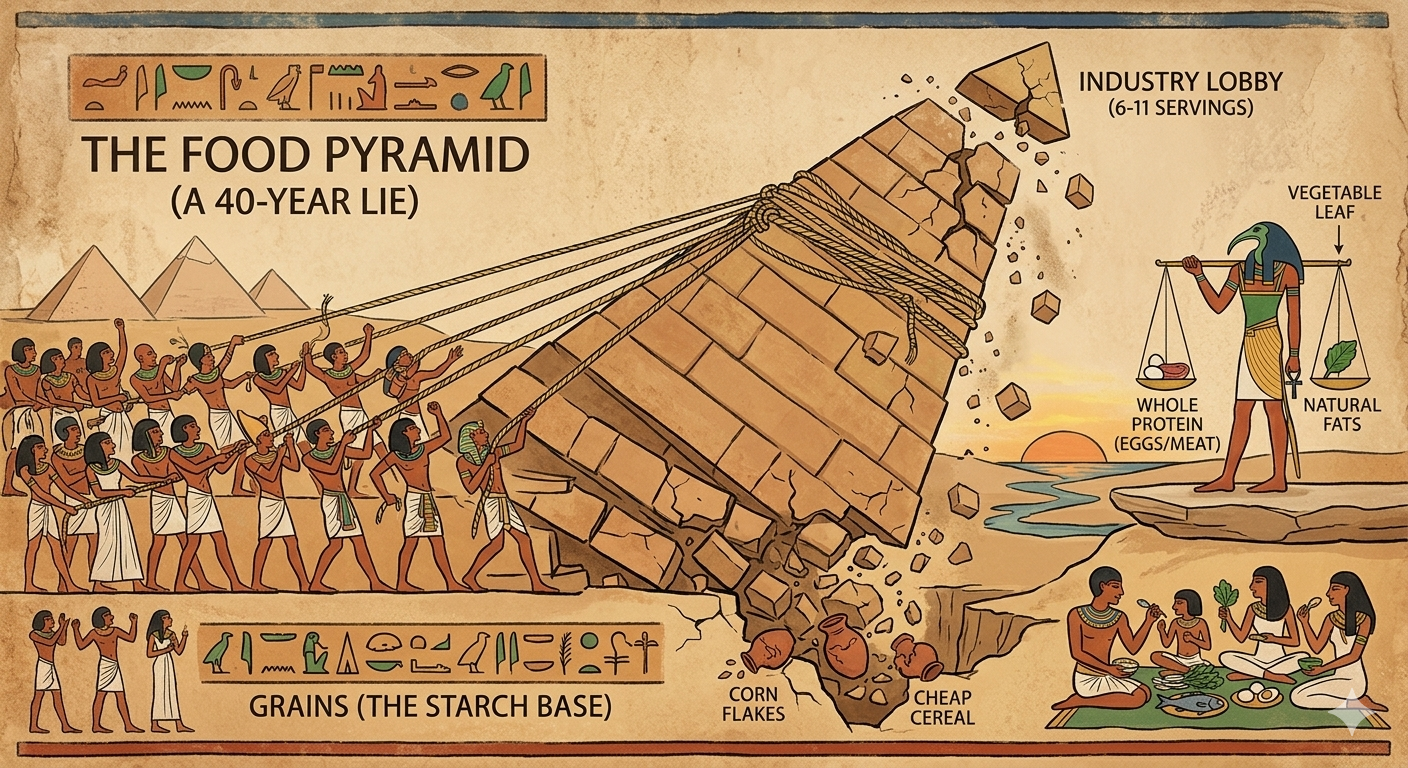
In a previous post, we tore down the traditional food pyramid and put it in the trash, alongside the myth that there are “good carbs” and “bad carbs” for Diabetics (hint – they are all bad!).
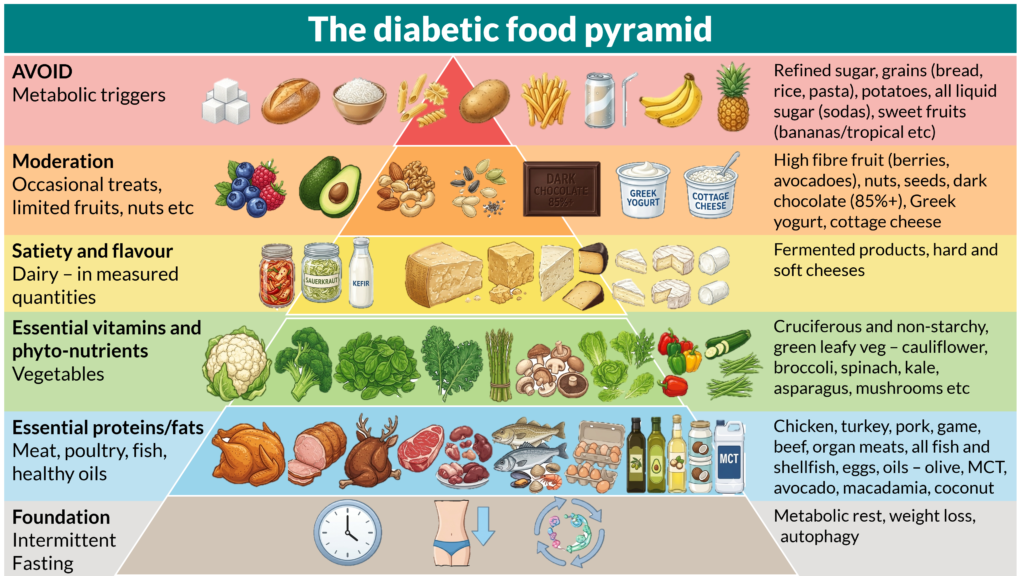
It’s never good to merely critique established “wisdom” without being constructive and offering a better alternative, so here is my proposal for a new diabetic-friendly food pyramid!
Let’s run through it layer by layer, starting at the bottom.
The foundation – intermittent fasting
My base or foundation layer supports the rest of the pyramid and is intermittent fasting.
Why so fundamental?
Fasting is the exact opposite of and therefore the natural antidote to Type 2 Diabetes!
For me, fasting is the philosophical starting point. In the simplest terms, the insulin regulation process that leads to Type 2 Diabetes is the fat storage process. The “trigger” for Type 2 diabetes is a breakdown in communication between insulin and your cells, usually caused by chronic energy overflow.
Insulin production is the regulatory mechanism for this excess blood sugar – when we have too much glucose in the blood, insulin is released to trigger the body to store the excess energy for later use. We all have a “set point” for how much energy (in the form of glucose) our bodies can tolerate before insulin cannot keep up.
Fasting is the inverse of that storage process. From an evolutionary standpoint, the reason we became very efficient at storing excess energy as body fat is so we could survive long periods of famine, which were common in our early development.
Fasting accelerates weight loss
Fasting is also my foundation for more pragmatic reasons. It’s a very powerful accelerator of weight loss. Weight loss occurs when there is a calorie deficit. Fasting is a very simple and effective way to achieve a calorie deficit. By reducing the window in which you eat, you can cut out one, two or even more meals in a day, thereby creating a significant calorie deficit.
In the past I lost a lot of weight using a 16:8 fasting schedule. This time around I was determined to achieve diabetic remission rapidly so picked a more aggressive fasting schedule, 3 x 36hrs. By not eating for three days a week I effectively reduced my calorie intake by around 1/5, creating a huge deficit.
But fasting works even better with a low carbohydrate or ketogenic diet. The two complement each other perfectly.
When you lower carbohydrate intake below around 30g of carbs per day, the body switches gears and starts the mechanism whereby your stored fat is converted back into fuel. This process is called ketosis. Fasting also uses this exact same process to keep you “fueled” even when you take on board no new fuel at all.
Alternative diet approaches that also reduce calories run into a problem that makes them less effective than keto / fasting. Even when calories are reduced, if carbohydrates remain moderate to high, your blood sugar level is constantly high, causing insulin to be released – and this effectively puts you in “fat storage mode”, not “fat burning mode”.
The human body cannot do both things at once, it is either “fat burning” or “fat storing”. If you are in fat storing mode, but you have a calorie deficit, the only way the body can deal with the deficit is to cannibalize muscle tissue.
When you are in ketosis / fasting your body naturally and easily uses body fat as it’s primary fuel.
“But we NEED to eat…don’t we?”
As long as we have stored body fat we can survive almost indefinitely via the “fat burning” process (with appropriate supplements). This has been demonstrated by many recorded, medically supervised extended fasts – most notably that of Angus Barbieri who fasted for an astounding 382 days, from June 1965 to June 1966, surviving on tea, coffee, sparkling water, vitamins, and yeast extract (Marmite here in the UK, which people dissolve in hot water – similar to using stock cubes or bone broth). Barbieri lost 276lbs of stored body fat in the process!
As we know, weight loss is one of the clinical recommendations for achieving diabetic remission and by leveraging the natural mechanisms of fasting we can lose weight rapidly.
While I certainly don’t recommend extended fasts like that of Angus Barbieri, or even the 36 hour fasts I use, shorter, intermittent fasts have been demonstrated to be just as effective. We all fast naturally overnight for between 8 and 10 hours, typically, sometimes longer. The key to successful intermittent fasting is to begin by extending this period.
If you typically finish your last meal at 9pm, then eat at 7am, this would be 10hrs of fasting. Simply extend your overnight fast gradually. Start by either eating your last meal an hour earlier or your breakfast an hour later for an 11 hour fast. Once this feels comfortable extend it by another hour, and another. Aim for at least 16 hrs in the first instance, effectively removing one meal entirely. This is excellent for weight loss.
If you can, I highly recommend pushing your fasting practice further and I’ll explain why in the next section.
The healing power of fasting
Intermittent fasting introduces metabolic rest. While you’re not putting more fuel into the system, your organs have nothing to do, and so have time to recover and repair from the damage done by diabetes.
In addition, longer fasts, above 16 hours, kick off a process in the body called autophagy. This is the body’s natural cellular repair mechanism. Perhaps counterintuitively, when you are fasting, your body works hard to make it more efficient by repairing and getting rid of dead cells. It actually makes perfect evolutionary sense – when hunger sets in, you need to be prepared to work harder to find food, so you need to be in the best possible condition.
In the context of diabetes, autophagy plays a key role in maintaining blood glucose homeostasis, particularly through the regulation of insulin secretion and sensitivity. Additionally, autophagy aids in preserving the survival and function of pancreatic beta cells by eliminating harmful proteins within these cells, which is vital for the prevention and treatment of diabetes. For more information see this article here.
Autophagy ramps up significantly when you fast between 18-24hrs so pushing your fasting has significant additional benefits.
So – in conclusion, fasting is our foundation, or our base, because it reverses the process that causes diabetes – runaway fat storage – while helping accelerate weight loss, and at the same time it helps balance the systems involved in regulating insulin.
It also clears the way for healthy eating habits as we’ll see in the subsequent layers of our pyramid.
The food pyramid layer 1 – essential protein and fats
The flip side of fasting is feeding! And of course this is absolutely vital since if you don’t feed yourself, you’ll (eventually!) fade away and we don’t want that!
The basis of what you eat should cover the essentials. Amino acids and essential fats are literally the building blocks of the human body. They are also your primary sources of fuel through both gluconeogenesis and ketosis. These two processes take consumed or stored protein and fat and convert them to usable energy.
This layer should represent as much as 75-80% of your daily calorie intake. Yes, that sounds a lot, but these are the essential building blocks. These foods are naturally very satisfying so will help you feeling full through the day.
Layer 2 – eat your greens – nutrients and fibre
The next layer of our pyramid is vegetables and fruit. But this is not a catch all.
Vegetables on the whole are nutritious, fibrous and relatively low in starch, which releases slowly, however, there are key exceptions which should be avoided by diabetics.
As a general rule, vegetables that grow above ground are best, while those that grow below ground are typically more starchy and should be completely avoided. For example, potatoes, sweet potatoes, squash etc offer little additional nutritonal value beyond empty carbohydrates.
Fruit is generally something to avoid due to the high fructose content, which is fundamentally equivalent to glucose.. There are a few key exceptions. Avocados are, of course, a fruit, and arguably a super food. Berries are are also highly nutritious but relatively low in sugar so can be eaten in moderation.
Just a quick note – while botanically classified as berries, bananas are high-sugar metabolic triggers and must be avoided. Also, another bit of fruit genealogy trivia, strawberries are in fact not classed as a berry but are permitted in moderation.
This layer should represent around 5-10% of your daily calorie intake. Most of these foods are relatively low in calories so this still represents a lot of volume, which helps keep you full.
Layer 3 – Satiety and flavour (dairy)
Dairy takes an interesting place in our pyramid, since it includes both protein and fats. But also can provide some carbohydrates (e.g. lactose as found in milk, yogurt etc).
Dairy is not a dietary essential, indeed there are many who are lactose intolerant and cannot tolerate dairy well at all, but for most of us, it can help provide flavour and satiety to support your journey.
Dairy is also not an all-you-can-eat buffet. As mentioned, lactose is essentially a sugar, and some dairy products have more than others. As a rule fermented dairy products like hard cheeses are much better than non-fermented products like milk and cottage cheese.
Also avoid “low fat” and “skimmed” versions of any dairy products – e.g. Greek yogurt. These versions have more lactose and therefore more carbs.
And as we have discussed elsewhere, consuming anything as liquid, such as milk or yogurt, rather than as a solid, makes the carbs much more readily available so will spike blood sugar more rapidly.
Cottage cheese and Greek yogurt are in my “moderation” list rather than their natural home in this category. Cottage cheese is actually not fermented, and effectively in a liquid form, and so Dr Richard Bernstein refers to it as liquid sugar, and advises avoidance.
Dairy should ideally represent no more than 5-10% of your daily calorie intake. It’s a flavour enhancer and there to help with satiety. It’s absolutely not essential so less or none is fine!
Layer 4 – Moderation (occasional treats once your diabetes is under control)
In this layer we have foods which have many potential nutritional benefits, but at the same time, can be very high in calories and/or carbohydrates and therefore may hamper your initial weight loss goals, or derail your attempts to remain in ketosis.
This list includes even superfoods like avocados due to their relatively high carb count. Berries also feature on this list, along with nuts and seeds. Dark chocolate should also be treated carefully, as well as Greek yogurt and cottage cheese. Personally I consider cottage cheese to be “forbidden” but only because I despise it! 🤢
This layer should therefore be considered as an optional additional layer to include only after you get your diabetes under control.
What does “under control” mean?
Dr Richard Bernstein, in his seminal book “The Diabetes Solution” argues that diabetics are entitled to exactly the same healthy blood sugar numbers as non diabetics. So your target should be a normal, optimal HbA1c – which would mean in the range 22-27 mmol/mol (4.2-4.6%). This may come as a surpise to many of you who’s medical team are advising you to aim for 48 mmol/mol (6.5%)!
Bernstein provides stark evidence in his book that glucose levels this high will still cause significant damage which over time will still lead to diabetic complications. Getting down to the optimal level is the only way to prevent further damage and diabetic complications.
Further, we have to remember that the HbA1c blood test, while valuable, is nothing more than an average taken over a three month period. It does NOT show the daily spikes you may be experiencing. He again advocates for an optimal blood sugar level throughout the day, which would be betwen 80-90.
Once again, the medical profession often advises patients that 120 or even 140 is “fine”, but Bernstein has demonstrated that even at 100, blood sugar is high enough to cause more of the damage that leads to diabetic complications.
If any of your “treats” or “moderate” foods are taking you above 90 then these really should not be part of your regular eating plan, and should be pushed down to the fifth and final layer of the pyramid – foods to avoid.
Otherwise, allowing between 1-5% of these foods should be fine.
Layer 5 – AVOID! Metabolic triggers that send you back to diabetic hell!
You will, of course, note that the pyramid has another layer at the pinnacle. This is what we should be eating the least of. I’d like to say “none of” but I know we’re all human, and occasionally for whatever reason “life gets in the way” sometimes. We may find ourselves at a social event where it’s just not practical/polite to bring your own snacks. For whatever reason, we shouldn’t beat ourselves up if we do eat from this layer, but if we’re doing so as a “treat” we’ve already fallen back into the trap that made us diabetic.
These foods are very high in sugar and, therefore, naturally addictive. They can also trigger memories of “comfort eating,” which can be psychologically addictive.
If we want optimum health, as diabetics, we should actively avoid everything on this layer as far as humanly possible.
Sadly, we often see this being taught to diabetics as “foods to eat in moderation”! This is just plain wrong!
These are all foods that will make your diabetes worse, leading to high blood sugar, inflammation, cardiovascular damage, hypertension, diabetic neuropathy, and retinopathy, and many more potential complications besides.
Sadly, this black list isn’t just “obviously evil” foods – the ultraprocessed foods and fast food junk that we should all know are metabolic triggers for diabetics.
This list includes almost all starches and grains – rice, bread, pasta, etc., as well as the fruits and vegetables high in sugar.
Fruits should be completely banned from our diet apart from avocadoes and berries, which should only be consumed in moderation.
As mentioned earlier, starchy vegetables, typically those that grow underground, are much higher in sugar and should be avoided – that includes potatoes, sweet potatoes, turnips, parsnips, and celeriac. While carrots grow underground and are relatively high in sugar, and are excluded by some, I choose to put these into my “moderation” category due to their other nutritional benefits.
The 99% rule
You may have heard people talk about the “80/20 rule” for dieting. 80% of what you eat should be healthy and nutritious and it’s fine for 20% to be “play food”. Ie whatever you want. I can tell you that I used to subscribe to this rule myself, and it’s a large part of what made me diabetic. The 80/20 rule is NOT appropriate for diabetics. Getting 20% of your calories from this group of foods would be absolutely disastrous.
I propose a new rule for diabetics, let’s call it the “99% rule”.
99% of what you eat should be from our four primary food group layers at the proportions listed (and presented at the end of this chapter in summary form), with 1% – a very occasional treat – coming from the forbidden list.
The 99/1 rule allows for things like the occasional birthday and holidays, without you feeling like you are risking a full return to your old habits, and without you incurring significant damage during the inevitable glucose spikes.
What does that equate to in real terms? I would argue that anything more than a single monthly slip into the forbidden list is risking a relapse. More than that, and it’s starting to risk becoming a habit.
Of course, everyone is different. My other advice about this would be to use a CGM (Continuous Glucose Monitor) to see what kind of impact your typical slips have on your blood sugar – for those that are genuinely high impact (taking you above 100), I’d say stick to even less than once a month. Even then, if your treats are taking you to 140 or above, I would say these should be reserved for annual one-off occasions. Perhaps Christmas dinner or Thanksgiving. But not both.
The good news is that many of these special occasions can easily be catered for while sticking to our food pyramid – simply avoid the starches, and fill up on proteins, fats, and plenty of vegetables.
If you find some of your favourite “forbidden foods” don’t spike your glucose too badly – let’s say taking you to 100 maximum – then once a month is probably reasonable.
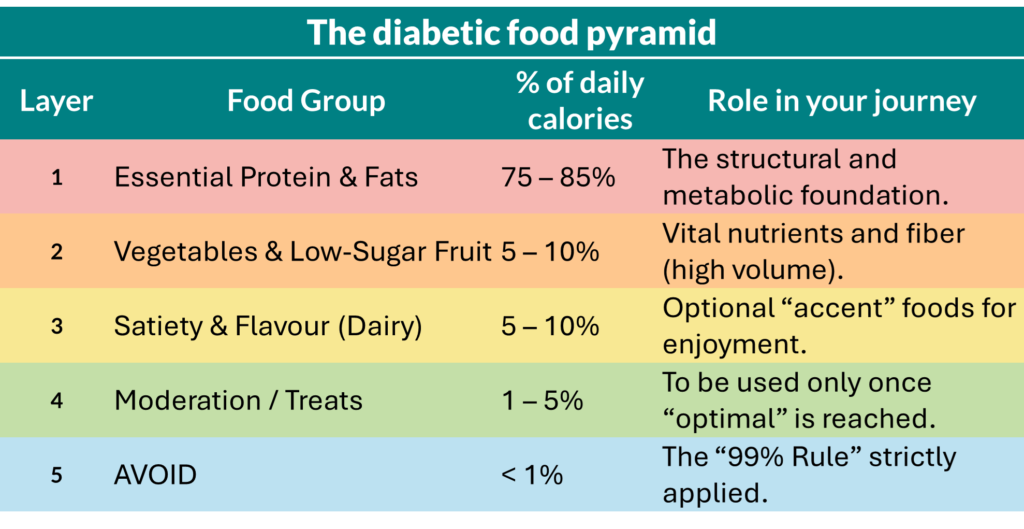
Summary
Let’s review the percentages of your daily calorie intake per layer again. You may have noticed, while going through the above, that if you stick to the top end of each calorie range, you’d end up over 100%! The math ain’t mathing! 😆
You need to think of these percentages as a sliding scale for your daily ‘metabolic budget.’ If you choose to enjoy the maximum range of dairy or treats, you MUST naturally dial back your protein and fat intake to stay within your total caloric goal. The foundation remains fixed, but the upper layers are a zero-sum game.
Also, we all have to accept that not all Type 2 diabetics are created equal. We all suffer from a degree of insulin sensitivity, some more than others. For some, even very small amounts of carbs as found in e.g., avocados and Greek yogurt may be sufficient to take your blood sugar over 90. Be sensible. If you want to eliminate the risk of blood sugar spikes, use a blood sugar monitor to see how your body responds to those higher-carb choices and adjust accordingly.
Likewise, if there are some of your favourite foods that might live in my “avoid” category, but you have verified that you can keep under 90 while eating them in moderation you can feel free to move them into your personal “moderation” layer. Just remember that you should periodically check your post-prandial blood sugar when eating these treats just to ensure that there hasn’t been any increase in your insulin sensitivity that warrants dialling them down, or even pushing them back to the “avoid” layer completely.
The aim of this pyramid is long term metabolic health – full diabetic remission with no risk of spikes that will lead to complications.
Some may read this and say I’m being a “killjoy” and that this is “extreme” and not “sustainable”.
All I will say to you is that I’ve had diabetic complications (chronic hypertension and severe neuropathy symptoms, along with early-stage retinopathy symptoms. And I can tell you that those things ARE extreme. Those things are a total “killjoy”. Those things are NOT SUSTAINABLE.
My opinion is that you will really want to avoid those things at ANY COST. And this may be the cost.
I, too, used to think this kind of way of eating was unsustainable, but all it took was 18 hours of persistent neuropathy symptoms to change my mind permanently.
And I don’t agree that these things “kill your joy”. As I’ve discussed elsewhere at length, the foods we love often don’t love us as diabetics. They are not “comfort foods,” they are toxic addictions. Removing toxic addictions from our lives should be a source of genuine joy and pleasure for all of us, and I can tell you that I feel so much happier now I’ve put them behind me.
If this is the price of long-term health and happiness, then it’s a price I, for one, am more than willing to pay.
I finally did it! After my recent three week plateau I have now broken through to 15 st 8.7 lbs (218.7 lbs / 99.2 kg).
In one fell swoop, I’ve smashed through the 220 lbs milestone AND that elusive but much more psychologically powerful 100 kg barrier!
I’m now into double figures metrically speaking! That feels fantastic!
This takes my weight loss since December to 2 st 11.2 lbs (39.2 lb/17.8 kg) and my total loss since diagnosis to 3 st 4.8 lbs (46.8 lb/21.2k g). I’ve now lost 17.63% of my original body weight at diagnosis, steadily approaching 20%! 20%!!! That will be 1/5 of my starting body weight!!! 😝
Progress Update: May 2, 2026
Week 19
HbA1c: 42 mmol/mol
Remission as of 30/03/2026
15 St 8.7 lbs
218.7 lbs / 99.2kg
Total loss (since December): 2st 11.2lbs (39.2lb/17.8kg)
Total loss (since Diagnosis): 3st 4.8lbs (46.8lb/21.2kg)
Exercise
Monday:
Run: 6×2.5min run / 1 min walk
No swim today due to tooth, run was fine
Tuesday:
GMB Fitness Mobility
First day – very challenging but successful
Wednesday:
Swim: 4x250m
Leisurely first swim back after tooth extraction, all good.
Thursday:
Run: 7x2min run / 1 min walk
Recovery run
Friday:
Swim: 2x500m, 1x250m (1.25km)
Shoulders started to twinge a bit so kept to 1.25km
Saturday:
Run: 6×2.5min run / 1 min walk, GMB Fitness Mobility 15 mins
20c heat for the run which was challenging, very proud to have completed GMB as well!
Fasting
Monday:
46 hr fast
Pushed 36 hour fast to 46
Wednesday:
36 hr fast
Completed successfully
Friday:
36 hr fast
Completed 3rd fast of the week successfuly!
Blood Pressure
Wednesday:
137/95 (65 bpm)
BP a bit higher again today
Thursday:
137/91 (70 bpm)
pretty consistent with yesterday
Target: 12st 12 lbs (180lbs / 82kg)
Remaining: 38.7 lbs / 17.6kg
55%
As you can see from my ticker above this means I’m now at over 55% of my weight loss target with just 38.7 lbs / 17.6kg left to go!
Confession time! Diet blips ahead!
I had a bit of a “diet blip” over last weekend. I went up to Newcastle to see my partner and she served up wholewheat pasta with bolognese on Saturday. I hate to put her out and make her cook separtely for me so I mostly ate around the pasta, but ate a little bit.
But then on Sunday we went out to the Everyman cinema. It’s something we used to do quite regularly, and a real treat was their Spielburger menu, where they serve really nice burgers, with sweet potato fries, right to your comfy sofa in front of the screen!
Given my recent successes, I decided to allow myself a minor lapse and enjoyed it immensely, although I could literally feel my blood sugar rising! It felt quite uncomfortable by the end. So it’s certainly not something I want to do very often, and I’m glad I felt some real discomfort as a reminder.
This was my third time seeing the (now not-so) new Ryan Gosling sci-fi movie Project Hail Mary, which has entered my top 15 favourite movies of all time – quite a feat given how much of a movie aficionado I am. It’s actually jumped above even Christopher Nolan’s Interstellar! I cannot recommend it highly enough. Unlike Interstellar, it’s a much less dark, more fun movie.
Anyway, following my lapse, when I came home from Newcastle, I decided to extend my usual 36 hr fast to a 46hr fast, skipping breakfast on Tuesday and not eating until the evening. That was my longest fast in the last three or four years. I expect to integrate a few more longer fasts over the coming weeks, since I’m now officially “unemployed”.
While I have been quite comfortable working during my 36hr fasts, I know that longer fasts can impact my energy levels/concentration so it’s a good time to stretch myself.
When you start to see plateaus, as I have recently, breaking up your schedule can be a good idea. For me, that means trying different fasting schedules. So I will push for a 48hr fast, and then the next step after that is a 56-58hr fast, basically fasting for two solid days, for example, from Tuesday night’s last meal, fasting all day Wednesday and Thursday, then breaking fast Friday morning. I may give that a go this week!
The rest of the week I was back to my strict keto diet and two more regular 36-hour fasts. It’s a testament to how well I’ve been doing that, despite pasta and burgers, I still lost a total of 2.5lbs (1.13kg) this week!
Of course, I do need to watch the temptation to fall back into old patterns. An occasional treat is fine; if it becomes a regular thing, it will only set me back. It’s not only about my weight; the most important thing is the need to keep my blood sugar under control.
My blood pressure has been fairly consistent this week, a little on the higher end of where I’d like it to be, but still within acceptable parameters.
This coming week, on Tuesday, I have my official GP diabetic checkup, which will include a new HbA1c, which I’m really excited for.
I’m anticipating that my trajectory for lowering my blood sugar to have continued since my last test at the end of March, and therefore expect to see a new HbA1c somewhere around 34–38 mmol/mol.
Of course, given my recent Chinese food, pasta and Everyman Spielburger “treats” I should anticipate a slightly slower trajectory – as the HbA1c is more sensitive to your recent blood sugar, and these lapses were all in the last month – but one or two meals in a sea of strict keto habits and 108-120 hrs of fasting each week is still just a drop in the ocean.
I am ultimately targeting a completely normal, healthy, non-diabetic HbA1c, which would be in the 23–27 mmol/mol range, so I still have a little way to go.
It’s worth noting that it is entirely normal for the trajectory/curve of metabolic transformation to slow and flatten out as you approach the “optimal” level, since the body has mechanisms in place to prevent your blood sugar from getting too low. That being said I still think it’s not unrealistic to anticipate getting to that target around the same time I hit my weight loss goal of 180lbs, which is mid to late September.
And I also anticipate along the way being able to drop my blood pressure medication entirely.
So that will be a complete metabolic transformation within 9-10 months – less than a year! I also intend to build my fitness up significantly by then, enough to break my previous personal best for a 5km run.
This will make me the fittest I’ve ever been in my life, as well as probably the healthiest, and certainly the lightest I will have been since I was around 21-22 years old – 35 years ago!
2026 is definitely going to be a truly memorable year! 😊
I’ve been hovering around the 221/22lbs (just over 100kgs) for over three weeks now, which represents my first proper plateau. I’ve had “setbacks” in the past where I’ve put weight on after losing it, but that’s always been with a clear explanation. A business trip, a birthday, Christmas etc. A plateau, for me, is when you are doing all the usual things (or think you are) and still manage to stall. Not necessarily putting on weight (maybe the odd 1 lb or less), but not losing either.
Generally speaking, when you experience these types of plateau it’s generally for one of the following reasons.
Water retention The most common, which we’ve seen through my blog, is that your body is simply holding on to water. We’ve discussed the mechanism before where fat cells can prove to be tenacious. Your body doesn’t want to just drop them entirely because creating new fat cells to store more fat when needed has a higher metabolic cost. So instead of dropping them it temporarily uses them to store water instead of fat. As you persist with your fasting and low-carb protocol, your insulin levels eventually drop low enough to signal the fat cells to release that stored water. This is what I call the “whoosh” effect. Nothing happens for a while, and then “whoosh” a big chunk of weight is gone. Persevering through these temporary delays is simply something you need to get used to.
Weight loss triggers BMR adjustment A second cause, albeit less common, is it can be a signal that you’ve reached a weight where your base metabolic rate (BMR) has reduced due to your successful weight loss to date. As we’ve long established, weight loss is fundamentally a function of a consistent calorie deficit, which we calculate based on your body’s metabolism. How much energy does the system need to keep it going through the day? As you lose weight and are maintaining a smaller frame, your BMR will drop. Not hugely, but potentially enough to stall your progress. It’s certainly worth revisiting the BMR calculator and just checking that your food intake isn’t outpacing your metabolism. Of course, this doesn’t happen every week – it’s usually something that happens after you’ve lost 20-30lbs or more. And usually your BMR hasn’t changed hugely – it could just be just a few hundred calories difference per day, but this adds up week by week and reduces your deficit, thereby potentially causing a stall or plateau.
A NEAT trick If you aren’t seeing an obvious change in BMR, it may be you are experiencing Non-Exercise Activity Thermogenesis, also called NEAT. When you are in a deep caloric deficit (like in my 36-hour fasting cycles), your body automatically becomes more “efficient.” You subconsciously stop fidgeting, sit more often, or move less during the day to conserve energy. This can account for a 200–500 calorie difference that won’t show up on a BMR calculator.
Stress and cortisol Stress can also lead to a plateau. When you are stressed, cortisol – the stress hormone – floods the system. Think of cortisol as a paranoid metabolic accountant. When you’re chronically stressed or underslept, this hormone convinces your body that a crisis is imminent, triggering a “lockdown” on your energy stores. Even if you haven’t eaten a single carb, cortisol triggers gluconeogenesis, where your liver creates and dumps glucose into your bloodstream to prepare for a “fight or flight” moment that never comes. This phantom sugar spike forces your body to release insulin, which we know is the storage hormone, that effectively locks your fat cells. You simply cannot burn body fat while insulin is busy policing a stress-induced sugar surge. Furthermore, cortisol is notorious for causing water retention and signaling the body to hoard fat specifically around the midsection to protect vital organs. You might be doing everything right in the kitchen, but if your internal “Emergency Accountant” thinks you’re under attack, it will override your progress to keep the vault closed.
Physical damage repair. I recently had a tooth extraction. This is another type of stressor that comes with its own challenges for weight loss. Repairing the site of the tooth removal requires increased blood flow, which in turn requires water. Your body will begin to store excess water to prepare for the “reconstruction”. Once the repairs are complete, any excess/unused water will be dropped. In addition, for diabetics, especially those of us taking supplements like Benfotiamine and ALA for neuropathy, a similar thing occurs as our nerves repair and blood flow improves to previously hypoxic tissues. Hypoxic just means deprived of oxygen – think of it like a kink in a garden hose. When the hose is “unkinked” there can be localized inflammation and increased blood volume. While ALA is generally weight-neutral or slightly helpful for loss, the process of metabolic repair can cause systemic water shifts that mask fat loss on the scale.
The “Pseudo-Plateau” of Body Recomposition Since exercise is an important part of my program, with swimming three times a week and running two to three times, I am also likely experiencing body recomposition. Muscle is almost 20% denser than fat. As I gain lean muscle mass in my legs from running, and shoulders and back from swimming, this will counteract some of the effects of losing fat. Even though muscle mass takes longer to build than fat does to lose, the scale will sometimes stay static while my visceral fat – which is the driver of T2D – is actually decreasing. This is why tracking your waist-to-height ratio and blood pressure is more important than the scale. If my BP is improving or waist-line is improving, the “plateau” is a lie and my health is still improving.
Hyperinsulinemia – stuck in fat storage mode, not fat burning There is another specific plateau that diabetics need to be aware of: Hyperinsulinemia. Even if your dietary carbs are zero, your body may still have high baseline insulin levels due to existing insulin resistance. Insulin, as you will recall, is the fat storage hormone and it literally prevents the breakdown of fat. Until your fasting insulin levels drop significantly (which lags behind blood glucose improvements), your body remains in “storage mode.” You might be “stalled” simply because your body is finally clearing the internal “clutter” (liver and pancreatic fat) before it’s willing to burn peripheral body fat again. Even though I have successfully dropped over 38lbs through a consistent calorie deficit my baseline insulin levels (fasting insulin) may still be significantly elevated, even though my blood glucose has improved substantially. Weight loss and blood glucose improvements usually happen faster than the reduction of insulin resistance. As a serial yo-yo dieter, hyperinsulinemia is the mechanism that has most likely stalled previous attempts at weight loss so it’s the one I need to be most aware of.
My current plateau experience
For me, I think I’ve experienced potentially a combination of a few of these plateau causes.
I’ve been stressed due to my recent redundancy, the “logistics” of which have dragged on, and I am now facing temporary unemployment and the stress of job hunting.
At the same time, I’m still recovering from my tooth removal last Friday. I think I’m now over the worst of this, which may help account for my progress this week – more on that in a second.
Of course, as a result of my tooth removal, I had to miss a few swim and run sessions, which would have temporarily lowered my metabolic needs, so even eating the same as I always have would result in a smaller calorie deficit, which can potentially stall weight loss.
At the same time, just before that, I had seen significant improvements in my swimming and running, as I consistently was able to increase speed and/or duration/distance. I can also see in the mirror and feel in my trousers that my midsection has toned up considerably. I now look quite buff from certain angles! 😊 So there is undeniable evidence of body recomposition.
Dealing with plateaus
The key to dealing with plateaus is twofold.
Firstly, be patient. Most plateaus resolve themselves naturally in a few weeks of consistent behaviour. You just need to trust the process. Certainly, it won’t hurt to review your portion sizes and see that you haven’t gradually been creeping up or adding things.
If a few weeks don’t start things moving, then generally the answer is to look at your calorie deficit. It may be that your weight has adjusted, or your body has become more “efficient” to the point where you need to lower your calorie intake in order to get to that next level.
Remember that it took many months and years of habits to get to your diabetes diagnosis. It will take a while for your body to recover. Give yourself time and have patience.





{kind=link}