When I was first diagnosed with type 2 diabetes, I knew very little about it, I was scared and confused, and learning about the disease, as well as some of the conditions that often accompany it, definitely helped put things in perspective. Ultimately, it was understanding the danger I was in that motivated me to change. This stopped being about weight loss for me, it was life and death stuff.
DISCLAIMER
I gathered this FAQ initially as part of my own self-education. This is gleaned from various sources over many years and should not be considered medical advice, nor should it be relied upon for accuracy. As I have said elsewhere, I am not a doctor and have no relevant medical training. Always consult your own practitioner before embarking on any serious changes in your lifestyle and especially your medication.
Under NO circumstances should you ever adjust your medication without first consulting your medical team.
Quick Navigation:
- What is diabetes?
- Redefining Type 2 Diabetes
- Other factors (Genetics)
- Type 2 Diabetes: Not just a “fatties disease”
- The pancreas
- Why the pancreas is the most important organ in Type 2 Diabetes
- Pancreatic cancer – not to worry you but…
- Do I need medication?
- Is Type 2 diabetes curable?
- Weight loss (The DiRECT study)
- Dietary change – the low carb verdict
- Intermittent fasting & Autophagy
- What about exercise?
- The quadruple whammy effect
- Simple isn’t easy
- HbA1c (The Snapshot Test)
- Daily blood sugar / Finger prick tests
- The sweet smell of (ketogenic) success
- Hypertension (The Plumbing Analogy)
- Symptoms of hypertension
- Reducing high blood pressure
- Orthostatic hypotension and cough syncope
- Insulin Resistance and the Kidneys
- Diabetic Neuropathy (Nerve Damage)
- Diabetic Foot Ulcer (DFU)
- Diabetic Retinopathy (Eyesight)
- Visceral Fat (The Hidden Danger)
- Glycemic Load (GL) vs Index
- Gluconeogenesis (The Body’s Generator)
- Why should I sign up?
What is diabetes?
The bad news – type 2 diabetes is a nasty, insidious, progressive disease that strangles you from the inside. It typically starts by attacking your circulatory system, clogging up your blood vessels and causing hypertension or high blood pressure. It then impacts your kidneys, nervous system, optic nerves and other key systems, and can lead to blindness, amputations and early death.
Diabetics are generally considered to have double the risk of mortality compared to those without. This, of course, is an average – obviously, the further the disease progresses, the higher your risks. For every 1% increase in HbA1c, (e.g. from 6% to 7% or from 42mmol/mol to 53mmol/mol) the risk of death from cardiovascular causes (heart attack/stroke) and kidney disease climbs significantly.
There are also strong correlations to be found between type 2 diabetes and pancreatic cancer, which remains one of the most deadly and untreatable cancers in the world.
The good news we are often told is that type 2 diabetes – unlike type 1 – is in large part a “lifestyle disease”!
“It is caused mainly by lifestyle choices – you eat too much sugar/refined carbohydrates/ultra-processed foods! Stop being such a greedy guts and get more exercise!”
But it’s not quite as simple as that, is it?
Redefining Type 2 Diabetes: Beyond the “Lifestyle” Label
The common characterization of Type 2 diabetes as a “lifestyle disease” tries to place the entire burden of the condition on individual choices, overlooking the profound environmental and systemic shifts that have occurred over the last few decades.
Evidence is on the rise that the growth of type 2 diabetes is closely tied to a food landscape that has been intentionally engineered for “craveability.”
Major food conglomerates deliberately adopted strategies from the tobacco industry, employing former tobacco scientists to apply hyper-palatability models to processed foods. These products are designed to bypass natural satiety signals, making it significantly harder for individuals to rely on willpower alone in an environment filled with addictive, low-cost options.
Furthermore, the physical reality of daily life has undergone a radical transformation. Our societal infrastructure has shifted toward increasingly sedentary working conditions and urban designs that often prioritize convenience over movement.
When addictive food engineering meets a mandatory decrease in daily physical activity, the resulting metabolic strain is a logical outcome of the environment rather than a simple failure of personal discipline.
Let’s reframe the conversation toward supportive solutions and systemic change rather than individual judgment. For further reading on these topics, I suggest the following:
Sedentary Work and Health: National Institutes of Health (NIH): The Impact of Occupational Shifting on Physical Activity
Food Engineering and Tobacco Influence: The Washington Post: How Big Tobacco’s Tactics Helped Create the Modern Food Industry
The Science of Hyper-Palatable Foods: University of Kansas: Research on the Tobacco Industry’s Role in Hyper-Palatable Foods
Other factors
There is a genetic predisposition to consider as well.
Unlike some conditions caused by a single faulty gene, Type 2 Diabetes is polygenic. This means it involves hundreds of small variations across many different genes.
- Heritability: Research suggests that the heritability of T2D – the proportion of risk explained by genetics—is between 20% and 80%. However, your family history can almost double your risk.
- Family History: If one parent has T2D, your risk is roughly 40%. if both parents have it, that risk can jump to 70% or higher.
- Beta-Cell Function: Many of the genes linked to T2D specifically affect how the pancreas produces insulin or how the body senses rising blood sugar levels
Type 2 Diabetes is just a “fatties disease” – isn’t it?
No, that’s not true. Not all type 2 diabetics are “fat” in the conventional sense. Around 10-15% of those diagnosed with T2D have a normal BMI.
It is more accurate to say that we all have a “fat threshold”, which is the limit of fat storage our body can handle before fat begins to accumulate in the liver and pancreas, leading to Type 2 diabetes. This explains why people of all sizes can develop the condition.
The Pancreas and the “Twin Cycle”
Why is the pancreas so important in Type 2 Diabetes? The pancreas has two critical roles, but in Type 2 Diabetes, it gets “clogged” by visceral fat.
- The Insulin Pump: The pancreas contains Beta cells that pump out insulin to manage your blood sugar.
- The Fat Clog: In Type 2 Diabetes, fat doesn’t just sit under your skin; it builds up inside and around the pancreas. Even a tiny amount of excess fat (as little as one gram) inside the pancreas can “stall” the Beta cells, stopping them from working correctly.
- The “Sleep” Mode: These cells aren’t necessarily dead; they are just “dormant” or overwhelmed.
How does the Fast Diabetes Reset help? This is where your 36-hour fasts and Ketosis come in.
- Clearing the Clog: When you fast for 36 hours, your body looks for the most “dangerous” fat to burn first. This is usually the visceral fat inside the pancreas and liver.
- The “Wake Up” Call: As that fat clears, the Beta cells can “wake up” and start producing insulin normally again. This is the biological mechanism behind Remission.
- Reducing the Load: By eating your low-carb menu (Keto Hana, Heck sausages, etc.), you are giving the pancreas a “holiday.” Because there is no sugar to manage, the pancreas doesn’t have to work overtime, allowing it to heal.
Why the pancreas is “The Most Important Organ” in T2D
In Type 1 Diabetes, the pancreas has failed permanently. In Type 2, the pancreas is usually just exhausted and smothered in fat. By adding this to your site, you move the conversation from “managing symptoms” (kidneys/blood pressure) to “fixing the root cause” (pancreatic fat). This aligns perfectly with the Newcastle University (DiRECT) study you mentioned earlier, which proved that losing fat from the pancreas is the key to reversing the disease.
Pancreatic cancer and type 2 diabetes – not to worry you but…
Diabetes is fundamentally caused by problems with pancreas function. When I was just 15 my dad died from pancreatic cancer (PC) – he was only 53 years old. So it was no surprise when I was diagnosed with Type 2 Diabetes that I I started doing some research into any possible link between PC and T2D, and yes, there does seem to be a definite correlation. It’s a slightly scary picture:
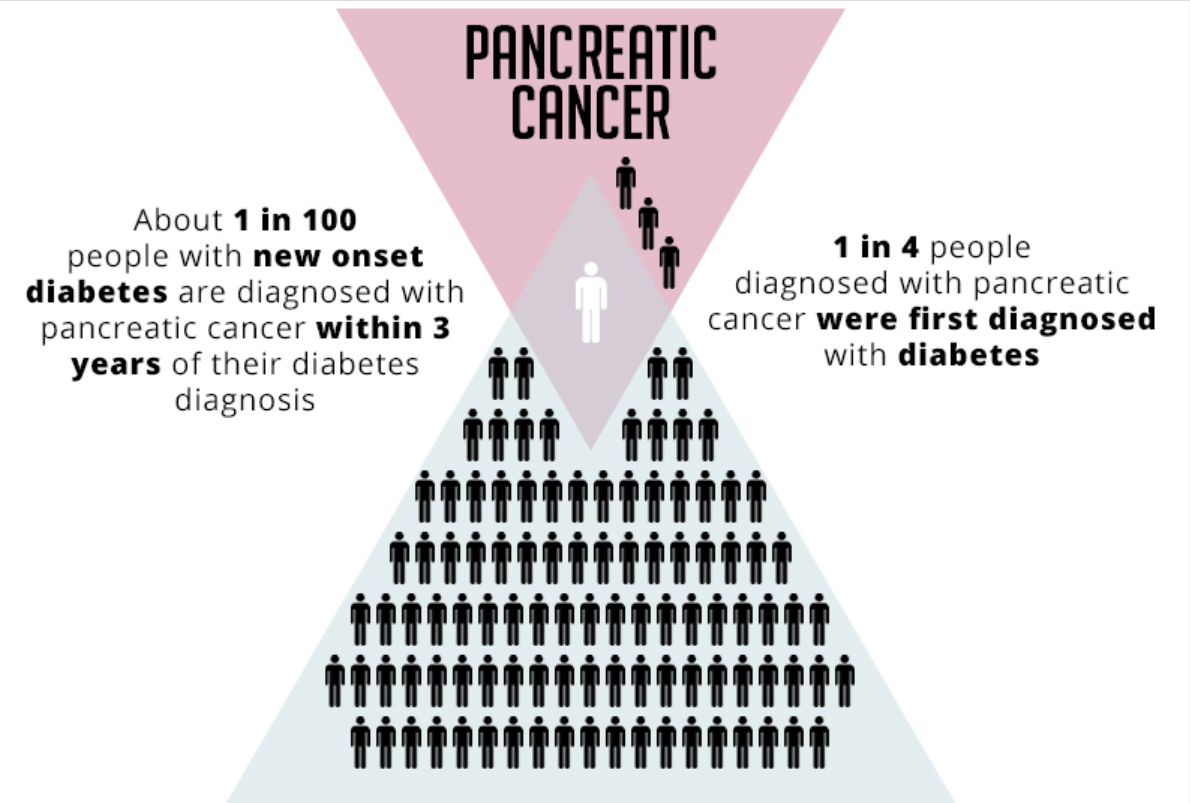
Those stats are from the following “interesting” article.
Living with diabetes for a long time “is a known risk factor for pancreatic cancer,”
V. Wendy Setiawan, Ph.D., of the University of Southern California
So, yeah, this suddenly got really, really real for me. Since my dad died when I was so young, I’ve had nightmares about going the same way. Pancreatic cancer is the deadliest cancer on the planet, with survival rates of just 25% beyond a year from diagnosis, and only 5% surviving more than 5 years. It’s very difficult to detect early, which is one of the reasons it’s so difficult to treat.
The good news is that given my family history of PC my GP took this very seriously, and investigated thoroughly to rule out any early symptoms of PC, which include jaundice, abdominal pain and sudden/unaccountable weight loss. An ultrasound also found no signs of the disease.
I mention this not to scare you but to advise you, if you have a family history of pancreatic cancer, do seek advice from your medical team.
Do I need medication to treat Type 2 Diabetes?
After a diagnosis of Type 2 Diabetes, you will often be offered medication. I am not a medical professional, so I cannot advise you here. But I asked my endocrinologist this question. Do I need medication to treat my type 2 diabetes?
His answer was “no, you do not. But you will need to make changes to manage it”.
This is a vital point. And, statistically, it’s a sad fact that most people with Type 2 Diabetes fail to make the necessary lifestyle changes to manage their condition. I struggled with this initially myself. I was determined, from the outset, that I could make the necessary changes and lose weight rapidly. I had done so before, and saw no reason why I could not do so again. So I point-blank refused medication.
While I initially lost some weight through fasting and increased exercise, I was then diagnosed with severe hypertension – critical in fact -, and it took 9 months before this condition was managed. During this time, I did not feel safe fasting or exercising, since both of these will increase my blood pressure. So my progress stalled.
By the time my blood pressure was properly managed, I had other personal issues, which made it challenging to focus on weight loss/exercise. It wasn’t until well over another year had passed before I was able to make the necessary changes, and by that point I had already begun to experience symptoms of diabetic neuropathy.
In hindsight, it does seem like I could have potentially avoided some of those symptoms had I started taking medication for my type 2 diabetes.
So I cannot simply say “don’t take medication,” even though I ultimately was able to achieve diabetic remission without any medication. The answer, as with many things in life, is “it depends”.
The benefits of diabetes medication (notably, Metformin)
In the UK, the first recommendation following a type 2 diabetes diagnosis is typically Metformin. Metformin is the “gold standard” for early diabetic treatment because:
- It doesn’t cause weight gain: Unlike some other diabetes drugs, it is weight-neutral or even aids in slight weight loss.
- Cardiovascular Protection: It has been shown to reduce the risk of heart attacks and strokes independently of its effect on blood sugar.
- Low Hypoglycemia Risk: It doesn’t force the pancreas to pump out more insulin (which can cause dangerous “hypos”); instead, it makes the body more sensitive to the insulin you already have.
Historically, doctors would wait 3–6 months to see if lifestyle changes worked.
Research showed that this “wait and see” approach led to years of slightly elevated blood sugar, which significantly increased the risk of nerve damage, as well as heart disease and kidney failure later in life.
Most modern guidelines now recommend starting medication at the same time as lifestyle advice to ensure the patient hits their target HbA1c as quickly as possible.
High blood sugar is toxic to blood vessels and nerves from day one. Doctors now prescribe medication immediately to “stop the clock” on damage while the patient works on diet and exercise. If the lifestyle changes succeed, the medication can be tapered off or stopped quickly enough. But the damage done by high blood sugar can be irreparable.
As mentioned, in my case, other complications arose that prevented me from making the necessary lifestyle changes immediately. Metformin would have limited the harm done while I was getting my hypertension managed by medication.
In hindsight, I should NOT have been so stubborn about avoiding medication. As you will see if you read my blog “life gets in the way”, far too often, and you should take every advantage you can get.
Is Type 2 diabetes curable? The good news
I also asked my endocrinologist this question: “Can it be cured/reversed?”. Clinicians are always reluctant to talk about “cures”. Once you have been diagnosed with Type 2 Diabetes, you will ALWAYS know that you have a propensity to the ill effects of the condition.
But the best news is that in most cases, Type 2 Diabetes can be put into remission, and purely by changes to your lifestyle. But please do not avoid medication like I did purely because you would prefer not to. While Type 2 Diabetes is very “simple” to treat with lifestyle changes, it is not necessarily easy. There is generally a reason why we develop Type 2 Diabetes, and that reason is based on years of ingrained habits. Changing these habits overnight can be challenging.
Give yourself the best possible chance to make those lifestyle changes by starting with Metformin, where offered.
The good news is that Type 2 Diabetes is quite well understood, with long term studies demonstrating the efficacy of three specific approaches. I won’t call them “treatments” since they are not. They are nothing more than lifestyle accommodations.
Weight loss
The Diabetes Remission Clinical Trial (DiRECT) focused on whether significant weight loss could actually “turn off” Type 2 Diabetes. The short answer. Yes, it can.
After 1-year of the study, 46% of participants achieved remission (HbA1c below 48 mmol/mol (6.5%)) which was then maintained without any medication. Remission was directly tied to the amount of weight lost. In the group that lost 15kg (33 lbs) or more, a staggering 86% achieved remission.
I mentioned this elsewhere, and I will say it again here. If you are recently diagnosed with type 2 diabetes, and have an HbA1c below 58 mmol/mol (7.5%), then you may well be able to reverse your type 2 diabetes by doing nothing more than losing weight. How you lose weight – in that case – is almost irrelevant.
If, however you have already gone above 58 mmol/mol (7.5%), already started to notice any other symptoms such as hypertension or nerve tingling (especially in the feet), or blurred vision, then I strongly suggest you stay for the rest of the story, because if you do not aggressively target your type 2 diabetes you risk permanent harm to your nerves and to your cardiovascular system.
Dietary change – the low carb verdict
Evidence from a 2021 review in Frontiers in Nutrition shows that low-carb diets (LCDs) can lower HbA1c even before any significant weight loss occurs. By limiting the primary trigger of blood sugar spikes (carbohydrates), you reduce “glycemic variability” – the dangerous highs and lows that damage blood vessels – independent of your waistline.
A 2024 study from the University of Alabama found that low-carb diets improved beta-cell function (the cells in the pancreas that make insulin). By giving these overworked cells a “rest” from constant glucose processing, they were able to recover and respond more effectively to meals, a benefit not seen as strongly in low-fat/high-carb weight loss diets.
The Diabetes Prevention Program (DPP) research has shown that “Diet Quality” (measured by the Healthy Eating Index) has an independent effect on diabetes risk.
If you lose weight by eating processed food, you miss out on fiber. Whole food diets, especially those containing high protein and fresh vegetables, produce Short-Chain Fatty Acids (SCFAs) in the gut. These SCFAs travel to the brain and liver to improve metabolic signaling and reduce hunger, providing a “hormonal” advantage that a UPF diet lacks.
Research published in The Journal of Clinical Investigation shows that nutritional ketosis – eating a ketogenic diet – can drop insulin levels by 50% or more within weeks. This “insulin holiday” allows the body’s cells to regain sensitivity to insulin much faster than they would on a high-carb, calorie-restricted diet. One of the most cited benefits in clinical trials (like those from Virta Health) is that ketones act as a natural appetite suppressant. This makes the calorie deficit required for weight loss feel “effortless” because it blunts the hunger hormone, ghrelin.
Micronutrients & Inflammation: Highly processed diets are high in trans fats and sodium, which cause oxidative stress. Even if you are thin, high oxidative stress keeps your body in a state of “low-grade inflammation,” which can keep HbA1c elevated even if your weight is “ideal.”
Meta-analyses (such as Choy et al., 2023) show that low-carb diets often lead to a more significant drop in triglycerides and a greater rise in HDL (good) cholesterol than low-fat diets, even when the total weight lost is the same.
A word of warning about medication: If you are currently on insulin or medications like Sulphonylureas or SGLT2 inhibitors, dropping to <130g of carbs can cause dangerously low blood sugar (hypoglycemia) or other complications. You must seek medical advice and work with your primary clinician to “taper” medications if you intend to lower your carb intake. DO NOT try a low carb diet while reliant on these medications.
Intermittent fasting
It’s important to understand that fasting isn’t just a way to skip calories; while this is certainly a mechanism that aids in weight loss, fasting also triggers a biological state called autophagy and a “metabolic switch” to fat burning similar to (but not the same as), that of ketogenic diets.
A study published in JAMA Network Open (2023) compared time-restricted eating (TRE or fasting) to standard calorie counting. While weight loss was similar, the fasting group showed unique improvements in insulin sensitivity. This is attributed to the extended “low-insulin window,” which allows the body to clear fat specifically from the liver more efficiently.
The “Twin Cycle Hypothesis” suggests that diabetes is driven by fat clogging the liver and pancreas. Research indicates that fasting protocols may accelerate the mobilization of this “internal” fat specifically, compared to a diet where you eat small amounts of sugar/carbs throughout the day, i.e., a typical ultra-processed foods diet.
Fasting for 16+ hours triggers cellular cleanup processes. While hard to measure in standard GP blood tests, this “housekeeping” is believed to reduce systemic inflammation, which is a major driver of diabetes complications like kidney disease and neuropathy.
What about exercise?
While exercise alone cannot reverse type 2 diabetes, the “magic” of exercise happens regardless of weight loss and diet. When you move your muscles, they pull sugar out of your bloodstream without needing insulin. This is known as insulin-independent glucose transport.
Studies show that as little as 7 days of vigorous exercise can improve blood sugar control by 45%—even if you don’t lose a single pound.
The Catch: This effect is short-lived. It begins to fade within 48 to 96 hours of your last workout. This is why consistency is more important than intensity for diabetes management.
What qualifies as “vigorous” exercise? Trust me when I tell you that it depends on where you are starting from! If you have never exercised a day in your life, then a brisk walk will be vigorous exercise! If you regularly play soccer then you may need to think about HIIT (High Intensity Interval Training). But I suspect if you regularly play soccer, you are less likely to be here with Type 2 Diabetes! 🙂
For me, I mostly swam, walked and did some walk/run interval training. I’m an experienced swimmer, but my weight precluded me from doing much running. I have previously injured myself from running, so have to be very cautious.
However, it’s worth noting that studies have shown that 75 minutes of vigorous intensity activity a week can give similar health benefits to 150 minutes of moderate intensity activity. So if you prefer to take it easy, 20 minutes of moderate exercise should be sufficient.
Moderate exercise options:
- brisk walking / hiking
- water aerobics
- moderate bike riding or swimming
- dancing
- mowing the lawn
Vigorous exercise options might include:
- running (walk/run schedules count!)
- swimming
- riding a bike fast or on hills
- stair climbing
- sports, like football, rugby, netball and hockey
- skipping
- aerobics
- gymnastics
- martial arts
If you have a sports watch or even an app on your phone that can measure your heart rate it can be good to use this to track your heart rate during exercise.
The important thing is the consistency of regular exercise is all that is required to help control your blood sugar.
The quadruple whammy effect
Weight loss, driven by a ketogenic diet and intermittent fasting, combined with the compounding effects of exercise, is a literal quadruple whammy, rapidly removing glucose from your system (changing the fuel), while giving your body the best chance to repair the pipes – i.e., to heal from nerve damage thanks to autophagy.
It really is that simple.
Simple isn’t easy
While that sounds simple – and I have certainly demonstrated that with my own success – that doesn’t necessarily mean it’s easy.
Cutting out sugar/refined carbs/ultra-processed foods is often challenging, as they can be our “comfort foods”. They were for me, and for many years they were the reason that my best attempts at losing weight always resulted in me eventually plateauing, failing, and giving up, before eventually returning to my old habits and my old weight.
But regardless of how hard you might consider it to be – I can only speak from personal experience and say that once you start to experience the complications arising from type 2 diabetes – nerve damage, eyesight issues, and hypertension, for example – you might be amazed at how easy it becomes to make radical changes to your lifestyle.
As the old saying goes “an ounce of prevention is better than a pound of cure!” It would be far better to motivate yourself to make these lifestyle changes now than once you are already experiencing serious symptoms.
HbA1c (glycated haemoglobin)
The primary test used to diagnose Type 2 Diabetes. Also referred to as glycosylated haemoglobin, haemoglobin A1C, or simply A1C. Glycated haemoglobin is something that’s made when the glucose (sugar) in your body sticks to your red blood cells. Your body can’t use the sugar properly, so more of it sticks to your blood cells and builds up in your blood. Red blood cells are active for around 2-3 months, which means the test effectively provides a “snapshot” or estimate of your previous 3 months’ blood sugar levels.
Very simply, a high HbA1c means you not only have too much sugar in your blood but have done so consistently for the previous 2-3 month period. This means you’re more likely to develop some of those diabetes complications we talk about elsewhere on this page.
It is therefore a much more reliable indicator of your blood sugar levels than the simpler blood sugar “pin prick” tests, which only show your blood sugar levels “now”. Pin prick tests are dependent on many factors and can change from hour to hour as well as day to day.
An optimal HbA1c level is 30-35 mmol/mol (4.9-5%). Outside of the optimal, the “normal” or “healthy” range is anything from 20-42 mmol/mol (4-6%). Anything above 48 mmol/mol (6.5%) is diabetic territory and generally considered a bad place to be!
An HbA1c level between 42 mmol/mol (6%) and 48mmol/mol (6.5%) is referred to in the UK as “prediabetes,” and while this is considered the first sign of trouble for someone who has never had diabetes, it’s actually the target for recovering diabetics to aim for.
Getting to 48 mmol/mol (6.5%) or below and maintaining it without medication for 6 months is considered “clinical diabetic remission”, at least here in the UK.
Interestingly, even though 42 mmol/mol (6%) and below is considered “healthy” or “normal” it is not the target for most diabetics, since there are potential risks in going from too high a blood sugar to under 42 mmol/mol (6%) rapidly – especially if you are taking medication to treat your diabetes.
Note that in my case, I never accepted diabetes medication, and so was not concerned when I blew past my target of 48 mmol/mol (6.5%) and hit 42 mmol/mol (6%) straight away after my first three months.
Update
Subsequent reading has revealed that what is considered “healthy” is really a misnomer. The table below represents a more realistic view of what is “optimum” for health vs the point where damage from glycated blood begins to occur (ie when too much sugar in the blood shows measurable harm to the organs, vascular system, brain and other parts of the body.
Credit to the Way of Reversing Diabetes (WORD) Facebook group for the data.
| HbA1c | Average blood sugar | ||
|---|---|---|---|
| % | mmol/mol | mg/dL | mmol/L |
| 4.0 | 20 | 65 | 3.6 |
| 4.1 | 21 | 69 | 3.8 |
| 4.2 | 22 | 72 | 4.0 |
| 4.3 | 23 | 76 | 4.2 |
| 4.4 | 25 | 79 | 4.4 |
| 4.5 | 26 | 83 | 4.6 |
| 4.6 | 27 | 86 | 4.8 |
| 4.7 | 28 | 90 | 5.0 |
| 4.8 | 29 | 94 | 5.2 |
| 4.9 | 30 | 97 | 5.4 |
| HbA1c | Average blood sugar | ||
|---|---|---|---|
| % | mmol/mol | mg/dL | mmol/L |
| 5.0 | 31 | 101 | 5.6 |
| 5.1 | 32 | 104 | 5.8 |
| 5.2 | 33 | 108 | 6.0 |
| 5.3 | 34 | 111 | 6.2 |
| 5.4 | 36 | 115 | 6.4 |
| 5.5 | 37 | 119 | 6.6 |
| 5.6 | 38 | 122 | 6.8 |
| 5.7 | 39 | 126 | 7.0 |
| 5.8 | 40 | 129 | 7.2 |
| 5.9 | 41 | 133 | 7.4 |
| HbA1c | Average blood sugar | ||
|---|---|---|---|
| % | mmol/mol | mg/dL | mmol/L |
| 6.0 | 42 | 136 | 7.6 |
| 6.1 | 43 | 140 | 7.8 |
| 6.2 | 44 | 143 | 8.0 |
| 6.3 | 45 | 147 | 8.2 |
| 6.4 | 46 | 151 | 8.4 |
| 6.5 | 48 | 154 | 8.6 |
| 6.6 | 49 | 158 | 8.8 |
| 6.7 | 50 | 161 | 9.0 |
| 6.8 | 51 | 165 | 9.2 |
| 6.9 | 52 | 168 | 9.4 |
| HbA1c | Average blood sugar | ||
|---|---|---|---|
| % | mmol/mol | mg/dL | mmol/L |
| 7.0 | 53 | 172 | 9.6 |
| 7.1 | 54 | 175 | 9.7 |
| 7.2 | 55 | 179 | 9.9 |
| 7.3 | 56 | 183 | 10.1 |
| 7.4 | 57 | 186 | 10.3 |
| 7.5 | 58 | 190 | 10.5 |
| 7.6 | 60 | 193 | 10.7 |
| 7.7 | 61 | 197 | 10.9 |
| 7.8 | 62 | 200 | 11.1 |
| 7.9 | 63 | 204 | 11.3 |
| HbA1c | Average blood sugar | ||
|---|---|---|---|
| % | mmol/mol | mg/dL | mmol/L |
| 8.0 | 64 | 208 | 11.5 |
| 8.1 | 65 | 211 | 11.7 |
| 8.2 | 66 | 215 | 11.9 |
| 8.3 | 67 | 218 | 12.1 |
| 8.4 | 68 | 222 | 12.3 |
| 8.5 | 69 | 225 | 12.5 |
| 8.6 | 70 | 229 | 12.7 |
| 8.7 | 72 | 232 | 12.9 |
| 8.8 | 73 | 236 | 13.1 |
| 8.9 | 74 | 240 | 13.3 |
| HbA1c | Average blood sugar | ||
|---|---|---|---|
| % | mmol/mol | mg/dL | mmol/L |
| 9.0 | 75 | 243 | 13.5 |
| 9.5 | 80 | 261 | 14.5 |
| 10.0 | 86 | 279 | 15.5 |
| 10.5 | 91 | 297 | 16.5 |
| 11.0 | 97 | 314 | 17.5 |
| 11.5 | 102 | 332 | 18.5 |
| 12.0 | 108 | 350 | 19.4 |
| 12.5 | 113 | 368 | 20.4 |
| 13.0 | 119 | 386 | 21.4 |
| 13.5 | 124 | 403 | 22.4 |
Daily blood sugar tests/finger prick tests – pros and cons
You won’t see any mention in my data of finger-prick test results, which I know type 1 diabetics swear by, as they can be life-saving. But I also know type 2 diabetics sometimes use them, and even non-diabetics engaged in ketogenic diets, wanting to track their blood sugar.
These types of tests are essential if you take insulin to treat your Diabetes, since over-medicating with insulin brings the literal risk of death.
However, these kinds of tests can also be highly misleading, since they only show your blood sugar at a precise moment in time. Blood sugar fluctuates throughout the day based on all kinds of factors, including, but not necessarily limited to, time of day, how well rested you are, general health, what you’ve eaten, and how recently. They can even swing based on you having a recent cold shower!
Since I never took any medication for my Type 2 Diabetes, I was never recommended to use such tests and have been very successful without them. Your mileage may vary.
I was ultimately driven by outcomes, and the primary outcomes I was targeting were weight loss and a lower HbA1c. The instant, limited-view “snapshots” provided by pin-prick tests were not useful in illustrating my progress towards those goals.
If you choose to use them and find them valuable for whatever reason, good for you!
On that note, I will add a slightly tongue-in-cheek alternative to checking your blood sugar…
Ketosis – the sweet smell of success
When you fast and / or follow a ketogenic diet, your body switches from burning glucose as its main fuel source to burning fat.
The Fat-Bank Audit
Think of your body like a high-interest savings account. When you eat carbs, you’re making constant deposits into your Fat Storage Bank. But when you fast or go keto, you stop the deposits and start making massive ATM withdrawals from your waistline.
Chemical money laundering
To make those withdrawals usable, your liver has to “launder” that stored fat into a currency called ketones. One specific byproduct of this transaction is acetone and acetoacetate – the chemical ‘receipts’ of your fat-burning success
Since your body can’t spend these byproducts, it tosses the receipts out through your breath and urine. Acetone is what you might smell in your breath. Acetoacetate is what you are primarily smelling in your urine.
Some ketogenic diet fans invest in what are called “keto strips” – small strips of paper covered in a chemical receptor sensitive to acetoacetate.
There is a fairly distinct smell that accompanies ketosis in your urine – some describe it as smelling a bit like nail polish remover. Learning to recognize the smell of these ketogenic byproducts in your breath or urine actually provides an alternative method of “tracking” blood sugar. While not necessarily reliable, as we have discussed, neither are pin prick tests, and as an alternative, it is completely free and doesn’t require drawing blood or aiming to pee on a paper strip!
Fortunately, I haven’t really suffered with ketosis breath, or at least not that anyone has pointed out to me! 😬 But I have learned to recognize the smell of acetoacetate very easily in my urine.
Eau de Adipose
So, the smell of ketosis could more aptly be called the “fragrance of fat loss”, or perhaps the French might call it “eau de adipose”! 😜
But ultimately, for me, it’s the sweet smell of success. It tells me that I am doing the right things, and keeping my blood sugar as low as possible.
When my pee stops smelling I know that I’ve somehow snuck in too much sugar and I’m now making glucose deposits rather than fat withdrawals.
Taking the piss
This has become a bit of a light hearted mantra for me – every time I pee I discreetly sniff just to see that I’m on track. When I get that telltale scent I smile to myself and think “ah! The sweet smell of success!” 👃🏼😁
Minor disclaimer – it has been noted that after many months of fasting, your body may become more efficient and stop “tossing the receipts away,” so the smell might fade even if you’re on track. After 4 months, I’ve not noticed this myself yet.
Just a word of caution: it may be wise to avoid sharing this particular bathroom ritual with your friends or coworkers if you value their continued company and respect!
And on a slightly more sombre note: This ‘sweet’ scent on the breath or urine is a sign of healthy nutritional ketosis for most Type 2 Diabetics. However, if it’s accompanied by extreme thirst, confusion, or vomiting, that’s an entirely different story – see a doctor immediately. While Diabetic Ketoacidosis (DKA) is very rare in Type 2 diabetics, it can happen if taking SGLT2 inhibitors like Dapagliflozin/Forxiga.
Hypertension
A very common symptom or co-morbidity of type 2 diabetes. High blood sugar causes inflammation and oxidative stress in the blood vessels, impacting your Endothelial System (aka the Vascular System).
The “endothelium” is the thin, inner lining of your blood vessels. Elevated blood sugar acts like shards of glass in the bloodstream, causing microscopic damage and inflammation to the lining. The Result: healthy blood vessels are flexible and can dilate (expand). Damaged vessels become stiff and narrow (atherosclerosis). Because the “pipes” are now stiffer and narrower, the heart has to pump much harder to move blood through them – this is the primary driver of hypertension.
I highly recommend ANY type 2 diabetes sufferer, whether diagnosed with hypertension or not, to invest in a home blood pressure cuff. Ensure it is medically approved in your geographical region.
I used this, the A&D Medical UA-611 BP monitor which is used by the UK General Practitioners Network. It’s available online and often sold in UK pharmacies. There are different models with additional features, but this is the most inexpensive, and I’ve found it to be very reliable. It’s battery-operated, using 4 x AA batteries. I have had this device since I was diagnosed with hypertension in July 2023 and have only changed the batteries once.

They are typically very easy to use and may have either an analog or digital display. The digital versions are generally easier to read and will provide heart rate as well as blood pressure readings.
While no device is ever 100% accurate, these are generally as accurate as the devices used by clinicians (and as mentioned, in the UK, these ARE the devices used by clinicians!) – the most important thing for tracking your BP is consistency.
Your blood pressure is recorded as two separate numbers:
- Systolic blood pressure is the first (top/upper) number. It measures the pressure your blood is pushing against your artery walls when the heart beats. Think of it as your active pressure.
- Diastolic blood pressure is the second (bottom/lower) number. It measures the pressure your blood is pushing against your artery walls while the heart muscle rests between beats. Think of it as your baseline or resting pressure.
Either a high systolic or diastolic reading can be used to diagnose high blood pressure.
The following chart is a quick and easy reference for tracking your blood pressure.
Note that either a high systolic or a high diastolic reading qualifies your overall blood pressure as falling into the noted category. So 120/84 is “normal,” but 120/85 is elevated. 139/86 is elevated, but 140/86 is mild hypertension, and so on.
| Stage | Systolic BP (mmHg) | Diastolic BP (mmHg) | Action |
|---|---|---|---|
| Normal and optimal | Below 130 | and Below 85 | Keep up the good work and stick with heart-healthy habits |
| Elevated | 130 – 139 | or 85 – 89 | Make lifestyle changes to lower blood pressure |
| Mild hypertension | 140 – 159 | or 90 – 99 | See a doctor or GP as soon as possible |
| Moderate hypertension | 160 – 179 | or 100 – 109 | See a doctor or GP as soon as possible |
| Hypertensive emergency | above 180 | or above 110 | Requires emergency medical attention. Go to a hospital |
Symptoms of hypertension
Hypertension often results in fatigue, and can contribute to other conditions such as erectile dysfunction in men, and generally requires medication to manage it until the diabetes is fully controlled.
Hypertension is widely referred to as “the silent killer”. Since the symptoms can be subtle, and easily attributed to other factors (stress, poor diet, physical effort etc), they can easily be missed entirely.
Failure to treat high blood pressure can lead to a stroke or cardiac event and even be fatal.
What to do in a hypertensive crisis / emergency.
If you do find yourself in the “hypertensive emergency/crisis” category, please try not to. While a hypertensive crisis is certainly a danger sign, panic will only make things worse. Pay attention to any other symptoms, such as shortness of breath, headache, blurred vision, confusion, or numbness/weakness and verify your blood pressure as follows:
- Sit quietly for 5 minutes. Do not talk, do not look at your phone. Ensure your feet are flat on the floor and not crossed at the ankles. Breathe deeply and easily. Take your blood pressure again only after 5 minutes have elapsed.
- Verify the Reading: Ensure the cuff is the right size and positioned correctly over your bare arm (not over a sleeve).
- Check for “Red Flags”: Ask yourself if you are experiencing:
- Severe chest pain or “tearing” sensation in the back.
- Sudden change in vision.
- Difficulty speaking or facial drooping.
- Call Emergency Services: If the second reading is still high and you have any of the red flags above.
Reducing high blood pressure
Your medical team will almost always treat high blood pressure with medication, but be aware it may take some time for them to find the correct dosage that manages your blood pressure without reducing it too far. While high blood pressure is dangerous, so too is low blood pressure as it can lead to fainting.
It took me almost 9 months of adding further medications and increasing dosage until my blood pressure was considered to be “managed”. This can be frustrating, but please bear with it and work with your medical team.
Ultimately, reversing your type 2 diabetes will see your blood pressure return to normal levels, and eventually you should expect to be able to eliminate all hypertension medication. But remember that this will also take time.
Think of it like this: Type 2 Diabetes is primarily an issue of fuel. The wrong type of fuel damages the pipes or plumbing. Too much fuel also causes harm to the plumbing, as increased weight adds strain to the system. This damage and extra strain all cause the pipes to thicken and, as a result, become less flexible.
Changing the fuel is relatively straightforward. It’s not quite as simple as a car, where you could drain the old fuel completely and refill with a nice new premium version! But remember that in normal operations, you would typically not empty the fuel tank completely before refilling, so some of the previous “old” fuel remains each time.
As mentioned in the HbA1c section above, it takes at least 3-4 months to see the old fuel completely replaced, even with a highly aggressive protocol like mine.
However, the damage to the “plumbing” is not automatically fixed just because you changed the fuel. The “pipes” (vascular system) will take more time, and it is a more complex system. While Type 2 Diabetes is primarily a metabolic issue (insulin/pancreas), hypertension is a multi-system issue involving your kidneys, your nervous system, and your heart.
Fixing the fuel issue resolves the insulin resistance, but if there is underlying salt sensitivity or if your kidneys have adapted to a higher blood pressure “set point,” they may still be signaling the body to keep pressure high. And as mentioned thicker, hardened arteries are less flexible and will take some time to return to their former state.
Don’t be surprised if your blood pressure becomes an additional challenge during your journey. See the next section for more details.
Orthostatic hypotension
For those with diabetes related hypertension, as you initially lose weight (typically around 10% of your starting body weight), the medication that you started on may prove to be too much for your system.
You will note that most medications have an “adult” and “child” dosage. If you are a pet owner, you will also have noted that most medications are based on your pet’s body weight. This is because medications have an “effective dosage” range based on how they are distributed through the body. A larger body requires a larger dosage. Too high a dose could be dangerous/toxic, while too small a dose will be ineffective.
As I mentioned, it took many months for my medical team to get my dosage correct, such that my hypertension was well-managed, in large part because of my larger body size. For obvious reasons, you do not want to suddenly increase the dosage beyond a healthy/tolerable level as this can lead to low blood pressure (hypotension – Note “hypo” instead of “hyper,” meaning under rather than in excess of) and fainting.
However, as you begin to lose weight, your body shrinks, and the dosage of current medications will eventually prove to be too much for you.
In those with hypertension, the first symptom will often be light-headedness, typically when standing or after effort. This is called orthostatic hypotension. Orthostatic hypotension occurs when your body is unable to maintain your blood pressure when moving from a recumbent (seated/lying) position to standing. You may experience this first thing in the morning or just when you have been seated for a while.
This occurs because of the damage to your “plumbing” we mentioned. Because your arteries have now become thicker and harder, they are less flexible, and an essential adaptation of the vascular system is to tighten the arteries in your legs as you stand up to “force” the blood back up to your brain. Since those with hypertension lose that flexibility, their ability to do this is compromised, resulting in a significant drop in blood pressure between being seated and standing.
A drop in systolic blood pressure of more than 20 points, or a drop in diastolic pressure of more than 10 points, is considered sufficient for a diagnosis of orthostatic hypotension.
In mild cases, the result is lightheadedness. In the worst case, a sudden drop in blood pressure may cause you to faint. If you are already mostly standing when this happens, you can of course, cause more serious injuries from an uncontrolled fall.
If you begin to experience these kinds of symptoms, you should take your time before standing up. Do so in stages. Sit on the edge of the chair/bed first and give yourself a few seconds to adjust before slowly standing. In the worst case, when you start to feel light-headed, immediately sit down or crouch as low as you can to limit any potential damage from a fall.
The key takeaway – it’s vital to keep an eye on your blood pressure medication, especially when you have lost between 10-15% of your starting body weight (as measured from your type 2 diabetes diagnosis). If you start to see signs of lightheadedness when standing, or after exercise, even if quite minor, that may be your signal to talk to your GP / primary healthcare practitioner about reducing your blood pressure medication.
Cough syncope
Coughing is another potential risk as your blood pressure medications become “too strong” for your system. Coughing actually places significant stress on your cardiovascular system, lowering your blood pressure and also leading to lightheadedness.
Persistent and/or severe coughing can result in a condition called “cough syncope”, where you lose consciousness. I personally experienced this and was lucky not to cause serious injury.
So do watch out for lightheadedness while coughing as well as standing.
Insulin Resistance and the Kidneys
High insulin levels can cause the kidneys to retain more sodium and water, increasing blood volume and further raising blood pressure.
Diabetic Neuropathy – nervous system damage
Once the circulatory system is compromised by diabetes, the reduced blood flow and high glucose can b egin to damage the nervous system, leading to diabetic neuropathy (numbness and tingling). The nerves furthest away from the heart and brain are the ones that are impacted first, leading diabetic neuropathy to be referred to as having a “stocking and gloves” or “socks and gloves” pattern. Ie, attacking feet and hands first.
If left unchecked, diabetic neuropathy can cause all kinds of complications. A serious potential complication of diabetic neuropathy is a diabetic foot ulcer described below.
Diabetic Foot Ulcer (DFU)
A serious complication where neuropathy (lack of feeling) and poor circulation combine to allow minor foot injuries to become deep, infected sores. Without the warning sign of pain, these can go unnoticed until they require intensive medical intervention or, in severe cases, amputation. Daily foot checks are highly recommended for diabetics for this reason. After a type 2 diabetes diagnosis, you should be scheduled for regular 6-monthly check-ups with your GP where they will test your feet for loss of sensation.
Diabetic Retinopathy – retinal nerve damage
Similar to the impact of raised blood sugar on the nerves of your hands and feet, diabetes also damages the blood vessels in the light-sensitive tissue at the back of the eye, called the retina.
At first, diabetic retinopathy might cause no symptoms or only mild vision problems, such as slightly blurry vision or less light sensitivity, but ultimately, this can lead to blindness if diabetes is not properly managed.
Visceral Fat
The ‘hidden’ fat stored deep inside the belly, wrapped around the liver and pancreas. Unlike the fat under your skin, visceral fat is metabolically active and secretes chemicals that drive insulin resistance.
While diet and weight loss will of course reduce visceral fat, exercise and activity have been shown to have a particularly strong effect here. By mobilising all of your major muscle groups, as in swimming, group aerobic sessions, dance aerobics, etc., you can significantly reduce your visceral body fat.
Glycemic Load (GL)
A measure that takes into account how much a food will raise a person’s blood glucose level after eating it. Unlike Glycemic Index, it accounts for portion size, making it a more practical tool for daily eating.
Avoiding high GL foods is essential for rapid type 2 diabetes reversal.
Is a Low GL / Low GI diet the same as a ketogenic diet?
No, they are not the same.
A Ketogenic Diet is a metabolic “reset.” It reduces carbohydrates so drastically (typically <25g net carbs per day) that the body switches its primary fuel source from glucose to fat (ketones).
A Low GI/GL Diet is a “slow-carb” approach. It focuses on carbohydrates that digest slowly to minimize blood sugar spikes, but glucose remains your body’s primary fuel.
Why Keto has the edge for Diabetics:
- Insulin Demand: On a low-GI diet, you are still reliant on your pancreas to produce insulin to manage those “slow” carbs. For those with high insulin resistance, this can keep you on a “mini-rollercoaster” – never quite reaching a stable baseline, which is needed for healing.
- Pancreatic Rest: By maintaining ketosis, insulin levels stay naturally low. This gives your insulin-producing cells a “break,” which is the primary driver in regaining insulin sensitivity over time.
- Visceral Fat: Keto is a powerful tool for targeting the fat stored in the liver and pancreas, which is often the underlying cause of Type 2 Diabetes.
The Strategy: Treatment vs. Maintenance
Think of the Ketogenic Diet as your primary treatment tool. It is the most efficient way to achieve rapid weight loss, lower HbA1c to normal levels, and reduce dependency on blood pressure or glucose medications.
I suggest viewing a Low GI/GL diet as a maintenance tool to be explored only after your health goals are met. By that point, the “long break” from high blood sugar allows your insulin sensitivity to recover. While Type 2 Diabetics must always remain mindful, achieving remission makes it possible to eventually reintroduce moderate, high-quality, slow release carbohydrates without the immediate “spikes” and long-term ill effects seen during the height of the disease.
Gluconeogenesis
The process by which the liver creates its own glucose from non-carbohydrate sources (like protein and the building blocks of fat). This is the body’s natural safety mechanism that prevents blood sugar from dropping too low during extended fasts.
While most of us might think “fasting” is little more than a strange religious practice, or a fad diet craze, it is important to understand that it is an essential part of our metabolism. We evolved over millions of years to survive periods of fairly extreme famine – lasting days and potentially even weeks – and so our bodies have become extremely efficient at storing body fat.
Because we don’t practise fasting regularly, however, our bodies become less practised and less efficient when it comes to burning that fat as fuel.
We all fast quite naturally overnight – it’s literally the reason we call our morning meal “break-fast” – and this will typically be between 10 and 14 hours between our last meal/snack of the night and our first meal the next day. By gradually increasing this fasting period, say to 16 hours, 18 hours or even longer, we train our body to become more efficient at burning fat.
The more efficient we become at burning body fat, it stands to reason, the faster we can lose weight.
See our fasting FAQ for more details.
The “Liver Spike” Mystery – “wait, why is my blood sugar HIGHER while I’m fasting?”
If you check your levels in the morning and see a rise – even though you haven’t eaten for 16 hours – don’t panic. This is often the “Dawn Phenomenon.” Your body is simply using Gluconeogenesis to “fuel up” for the day by releasing a controlled amount of glucose into your system.
Think of it this way: Eating carbs is like a home invasion of glucose that your body has to fight off. Gluconeogenesis is your liver acting as a smart thermostat, providing exactly what you need from your own fat stores. A rise from GNG isn’t a failure; it’s proof that your internal machinery is working exactly as it should!
Final Question – now I know how to do it why do I need to buy your Book?
“Hey – great FAQ, but you just told me exactly what I need to know! So why would I need to subscribe?”
The simple answer is – you don’t!
If you, like me, are a self-starting data-driven individual you can probably figure out the rest of it for yourself.
So what would you get by purchasing?
This is one FAQ, distilled from the core material in my book. That material was developed over the course of over 270 blog posts, across 8 years, during which time I documented my original forays into intermittent fasting, my experiments, successes and failures. Fasting is not something to enter into lightly and without proper guidance. Nor is a ketogenic diet.
I also had a number of previous successes with ketogenic diets which aren’t documented in my blog, as well as years of endurance and triathlon training, all of which informed my current and rather more detailed step-by-step plan, focused on the realities of “what happens when the rubber (literally) meets the road”. This includes things like exercising while in ketosis, adjusting for aging bodies, and so on.
My current real-time documentation of this specific success story started in December 2025 and discusses the initial teething troubles I had when getting back into fasting after a break, along with my simplified ketogenic diet, how I dealt with the holiday season, injuries, illnesses, setbacks, personal and professional issues, and so on.
While many “health gurus” will sell you on how easy things are, I cover all of the challenges I faced, often in nitty-gritty detail, and provide feedback on what worked for me as I overcame them.
In addition, purchasers of the book will have direct access to me via e-mail, so I can also provide real-time advice and guidance to supplement the material in the book and personalise it. Sure, there are plenty of support forums out there for Type 2 Diabetics, but many of them are populated by diabetics who are clearly resigned to a life of chronic acceptance of their condition. Many are sharing frankly bad advice about “good carbs vs bad carbs”, as well as incorrect information about fasting and the ketogenic diet – it’s simply not going to help you along your journey.
As a busy executive, living alone, I had to cook from scratch and find shortcuts to making weekly meal plans that worked and were repeatable (as well as being tasty! I can’t promise my taste will be the same as yours, but I’ll ensure that as you experiment for yourself, you keep the right principles in mind.
So sure, you can definitely figure it out for yourself, just like I did. Will you do it quicker with an experienced guide who has taken the journey before you and knows the paths intimately? And will likely entertain as well as inform and support you? As well as provide direct support along the way?
Would it be worth parting with a little bit of your hard-earned cash in order to have such a guide?
Only you can decide! 😊